Well, now. Interesting developments in the last few months, which have led to somewhat less writing.
Personally, I’ve been promoted at work. I am now the “Medical Director for Utilization Management”. This means a couple of things. Personally, it means a lot more work; as yet, I have no one to take over the actual “utilization management” I’m doing, so I do that and work the management in the cracks, or neglect the UM and do the management stuff. It also means I get tapped for a lot of committee work. A lot of it. Apparently there are parts of the organization that have been waiting for this nob to be created, and now I’m in it, they want me to fix their particular problem. (As in medicine, sometimes I say “That’ll get better with time”, and sometimes I say “That won’t ever get better, suck it up”. Sometimes I can fix it.
Professionally, I’m in a whole new neighborhood, and am running very quickly to keep abreast of my new responsibilities. While still dong all of the above. We now quote from my esteemed colleague at Monkeybagel.com:
Managing [physicians] is like leading a neighborhood gang of neurotic pumas on jet-powered hoverbikes with nasty smack habits and opposable thumbs. Oh, and as a manager you're a neurotic junkie puma too, only they cut your thumbs off and whereas all the other pumas get to drive around on their badass hoverbikes and fire chainguns at the marketing department, YOU have to drive a maroon AMC Gremlin behind them and hand out Band-Aids and smile a lot, when all you're REALLY thinking about is how to get one of them to let you borrow his hoverbike for a few minutes so you can show those fools how it's DONE. This is because managers are usually people who proved that they were handy with a chaingun and were thus rewarded by having their thumbs cut off and their weapons handed to some punk [new] hire.
Yeah. I admit few equals with a chaingun, and I’ve fired my share of grenades at marketing, or management, or whoever the target of the day was. (Perhaps more than my share; I was not above stealing someone else’s grenades, if I didn’t think they were shooting fast enough). And I’ve learned how management defends itself. They’re like the Borg: they assimilate you.
But I digress, because none of that has anything to do with the title of the post, now does it? In other professional news, I’ve been appointed to the Governor’s Opiate Emergency Task Force. This came about because the Massachusetts Association of Health Plans (hereafter MAHP) needed a representative with at least some “subject matter expertise”. So they called around, apparently also calling my uberboss, who thought of me (nice of him, I thought). He called asking if I was interested in doing this, particularly given my general level of overcommitment.
Well, this is the kind of opportunity which does not come along daily, so hells yes I’ll do it! Of course, this appointment did not come with any additional free time, naturally, so I’m doing the work for this in between the other work I’m doing, which you may recall I was doing quite a bit of that in between other work I had already been assigned to do. So, I’m a bit busy; a bit busier, even than most new managers who are learning a whole new skillset. I suspect it’ll be worth it, in the end, since I’m convinced the governor, like most people, is a bit late to the “opiate emergency” party; there’s been an “opiate emergency” since at least 2009, and possibly since the turn of the century. Here, have a graphic:
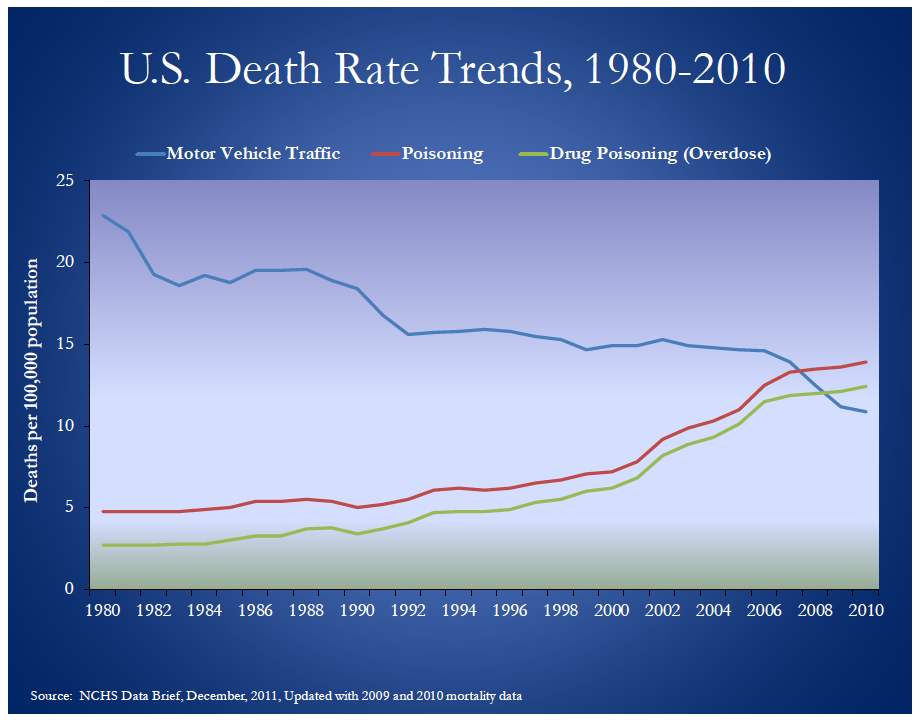
What you’re seeing here is the death rate for various causes, showing that “poisoning” (which is the category opiate overdoses go in) overtook motor vehicle collisions as the most popular cause of death in 2009. The discerning reader may note that the overdose death rate pretty much began to rise in the 90s; if you’re looking for when the “opiate emergency” started, that’s the place.
So, with luck we may find, not a solution, but a better stopgap, than we have right now. At least, that’s what I’ll be working towards. There are dozens of simple solutions which will not work. (More treatment! Less insurance regulation! Ban Zohydro!). A solution which will work will be a combination of prevention and treatment; neither will work in isolation. Personally, I like more prevention; others with a different view like more treatment (parents of addicted children, for instance). But you cannot do just one thing.
Stay tuned.